Reflection from Genève Excursion (8- 11 October 2025)

The Global Health Fellows internship provided me a once-in-a-life-time opportunity to practice first-hand class taught concepts under the guidance of Prof. Anuj Kapilashrami and the entire team. Through it, I have participated in global health projects within the Centre, contributing to research and evidence synthesis on migration health governance where I mapped actors and instruments.
The excursion in Geneva was the highlight of the internship experience, providing an opportunity to visit UN organisations such as World Health Organisation and International Organisation for Migration (IOM) which are central to global health governance. It was well-planned with a detailed itinerary that allowed us to interact with specialists in various global health areas such as Migration Health, Sexual and Reproductive Health and Infectious diseases. Learning from them and getting an opportunity to ask questions on their work and current challenges they are facing in light of the development aid cuts, massive layoffs and organisational restructuring. The sessions on migration health revealed how necessary the work I was doing at the centre was, uncovering the importance of safeguarding the rights of migrants, especially the right to health.
The global health landscape has been experiencing unprecedented challenges from the COVID-19 pandemic, rising humanitarian crises to most recently development aid cuts. This excursion therefore also came at such a crucial time for global public health students and early career practitioner providing first-hand experience to the impact of these challenges at the highest levels of global health governance.
Day 1
The visit to the International Red Cross and Red Crescent Museum explored the history and evolution of humanitarian aid, and the central role of the IFRC in it. The holographic accounts and testimonies, and various displays created an immersive experience highlighting the role of IFRC. Of note was its role in family reunification and reconstructing family links, with a dedicated wall of pictures of children separated from their families during the Rwanda Genocide (the pictures of the children were taken in a bid to reunite them with their families). A particular section was dedicated to the Holocaust, with IFRC taking accountability for failing react robustly and in a timely manner to it. Ironically and unfortunately, the world finds itself in a similar predicament with devastating crises such as the genocide in Gaza, with organisations and nations taking a neutral stance and failing to react to stop it.
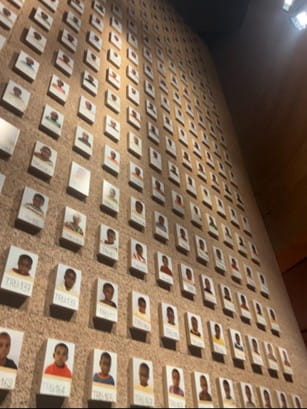
Image: Photographs of children separated from their parents during the Rwanda Genocide.
Day 2
The session with Doreen highlighted the normative role of the WHO, especially in policymaking and norm-setting. Respect for countries’ sovereignty was noted as a barrier to the adoption, implementation and enforcing of instruments such as treaties and protocols by WHO, with ratification not always amounting to implementation. Diplomacy was emphasised as an important tool in ensuring that countries commit to agreements stipulated in the various instruments, overcoming conflicts of interest and ensuring collaboration in addressing public health challenges. However, the time-consuming nature of diplomacy due to the competing country interests and complexity of multistakeholder interactions may result in delayed effective responses to health crises with exacerbation of health inequalities. The WHO Framework Convention on Tobacco Control (FCTC) was noted as a pertinent example of WHO moving beyond voluntary recommendations to setting obligations that are enforceable, supported by monitoring and reporting on compliance. Additionally, it provided a blueprint for WHO taking on commercial actors whose activities harm public health, yet are capable of influencing policy in favour of their commercial interests.
The second session was with Christina Pallitto and Hanna Mari from the Sexual and Reproductive Health and Research unit (it has been extended to include Maternal, Newborn, Child, Adolescent Health and Ageing). An overview on their work in combating female genital mutilation, including research and evidence generation. Of note was the FGM health cost summary that provides an evidence base to support interventions against FGM, showing that it cost $1.4 billion to treat FGM complications including obstetric complications that may increase maternal and neonatal mortality. People-centred approaches, including in communication, were also highlighted as a transformational way to advance prevention of FGM. It prioritises clear, culturally sensitive, respectful communication between health providers and patients, and active participation of patients, empowering them to have a say in their own health decisions. The session also explored how SRHR are under attack, facing compounded challenges resulting from the Global Gag Rule being enforced in addition to aid cuts. This limits access to information and SRH services robbing individuals especially women and girls of autonomy in making decisions concerning their bodies, with those living in precarious conditions such as conflict zones (DRC) suffering the most impact.
One of the most pressing global issues is migration and migration health, due to its current scale in light of rising climate change, political and economic instability and insecurity as drivers. Migration is now viewed as a determinant of health due to the impact of human mobility on migrants and their health, especially when it occurs under precarious conditions that worsen migrant vulnerabilities. The rise of populism and anti-immigrant rhetoric hidden behind health security to justify restrictive immigration policies further exacerbates challenges migrants experience, limiting their access to health and social services. The session on migration health highlighted these issues, with Claudia Marrota informing us that the division had been scrapped out altogether (removed from the WHO organogram), only to be brought back under a different division (Environment, Climate Change, Migration and One Health) with far less funding and expert human resources. These hampers efforts promoting migrant- sensitive health systems with migrants experiencing widening inequalities. Additionally, she noted other system level barriers such as “low quality evidence” arising due to lack of a common definition of ‘migrants’ which varies based on context and country’s laws leading to different variables collected that are difficult to collate.
The session at the International Organisation for Migration (IOM) at the IOM headquarters was led by Aleksandar Arnikov, who overseas operations of their Migration Health Division. He highlighted the role of the division in migrant health including conducting pre-departure health assessments, public health for people on the move, public health in emergencies and mental health and psychological support for migrants. While the first function is commissioned by host countries and runs parallel to their health system, the last 3 functions are focused on strengthening the health systems of host and origin countries. Community mobilisation and migrant networks within the communities they serve were noted as central to implementation of IOM activities, including disease surveillance and notification. Of interest was the displacement tracking matrix, a tool developed to assess mobility patterns and changes, which is dependent in a community informant. The lack of culturally appropriate services and health providers being unaware of migrant vulnerabilities were highlighted as access barriers. IOM’s funding largely (over 60%) is project-based, unlike other UN agencies that depend on voluntary contributions, thus IOM’s operations, while have been impacted by the global aid cuts, have not been undermined as severely. This funding model also accords it a level of operational flexibility within projects allowing it to respond to various migration crises as need arises. They also noted receiving funding from private actors such as Novo Nordisk, which highlights the importance of leveraging public private partnerships to advance migration health especially due to the ongoing aid cuts. However, navigating potential conflicts of interest can present a challenge.
The famous monument to mark the eradication of small pox, was great reminder of what concerted efforts across all nations, and global health collaboration can achieve in improving the health of all.

Image: Monument to the eradication of smallpox.
Day 3
The sessions focused on the role of WHO in infectious disease (control and prevention). The first presentation outlined current WHO efforts in eradicating polio by Oliver Rosenbauer, and current challenges they are experiencing. Polio remains endemic in part of Pakistan and Afghanistan, with operational (banning of house-to-house campaigns), technical (vaccine delivery to remote communities- challenges preserving vaccines) and political challenges (political instability and insecurity in Taliban controlled regions). Moreover, globally, the anti-science antivaccine rhetoric on the rise globally is also causing increased vaccine hesitancy and potential resurgence of polio in areas it was previously eradicated. Similar to other sessions, community organising was highlighted as an importance driver to advancing eradication efforts (women involved in vaccination efforts in Afghanistan). Failure to eradicate polio is a defeat for society.
Dr Tauhidul Islam took us through the session on Tuberculosis. This presentation was particularly unique as it framed TB as a social disease requiring a holistic approach that combines both upstream and downstream factors to effectively combat. The END TB strategy also situates TB eradication within the sustainable development goals, with economic and health development highlighted as mutually enforcing to increase the chances of developing sustainable TB solutions. Moreover, he also highlighted that overall strengthening health systems is paramount to eradicating TB.
The day proceeded with a guided tour of the United Nations Office where we were taken through the history of the UN from its development initially as the League of Nations led by President Woodrow Wilson. I was particularly intrigued by the tree from Hiroshima that survived the atomic bombing, and symbolises resilience, life and peace and the world’s ability to bounce bank even from the worst tragedies. Additionally, the beautiful art pieces in the form of paintings and sculptures that adorned the hallways of the Palais des Nations were a great reminder of the use of art as an agent of peace and tool for development.

Image: Artwork from the Palais des Nations.
Day 4
A self-guided tour of European organisation for Nuclear Research (CERN) concluded the activities of the excursion. I was fascinated to learn of the history of development of the world wide web which revolutionised communication and information-sharing globally, which are important in global health as it allows collaboration and knowledge exchange globally. It was also interesting to learn that the software was released into the public domain royalty-free allowing its global adoption and expansion by removing financial and legal barriers. This is contrary to the current technological innovations, which are heavily commercialised and may widen inequalities, even when they could potentially address global health challenges.

Image: Rebecca Adut Dau at CERN.
The uncertainty in the global health space and job market for early career public health practitioners was made apparent during the excursion. However, it also highlighted that there are still pertinent challenges to resolve that will require the knowledge and expertise I have gained so far, through the MSc Global Public Health (MSc. GPH) program and this internship, to solve. Therefore, the excursion provided assurance and confidence that I am in the right profession. I highly recommend that this experience be afforded to other MSc. GPH students as it will motivate and encourage them that their work matters and can have impact positive impact on global health.